The organization must give this signed and completed form to the Medi-Cal Dental. The Medi-Cal fee-for-service program adjudicates both Medi-Cal and associated health care program claims.
Https Www Dhcs Ca Gov Formsandpubs Forms Forms Mced Mc Forms Mc380 0618 Pdf
Apply for CalFresh.
Medi cal authorized representative form. Choose anyone that I wish to be my authorized representative. California medi- cal authorized representative form The National Health Networks General Purposes Policy policy is developed to assist the health network in managing program benefits and determine whether a particular procedure drug service or provision is medically necessary. If you need to install or upgrade to the latest version click the Download Free Readers.
Your authorized representative may assist you on duties noted below related to Medi-Cal Dental. Authorized Representative 41 Definition of an Authorized Representative 63-4026 An authorized representative AR is an adult non-household member who is authorized to act on behalf of a household in one or all of the following capacities. Medi-Cal Eligibility Division forms are listed alphabetically below by form number and may include alternate languages if available.
Authorized Representative Standard Agreement for Organizations This standard agreement must be completed by the person or persons who will act for the organization that the Medi-Cal Dental Program member has appointed as an authorized representative. Or you may also limit duties. PDF documents require Adobe Reader.
Box 15539 Sacramento CA 95852-1539. MCAP is also available to women who have other. Medi-Cal Page 4-1 Update 19-10 CalFresh 4.
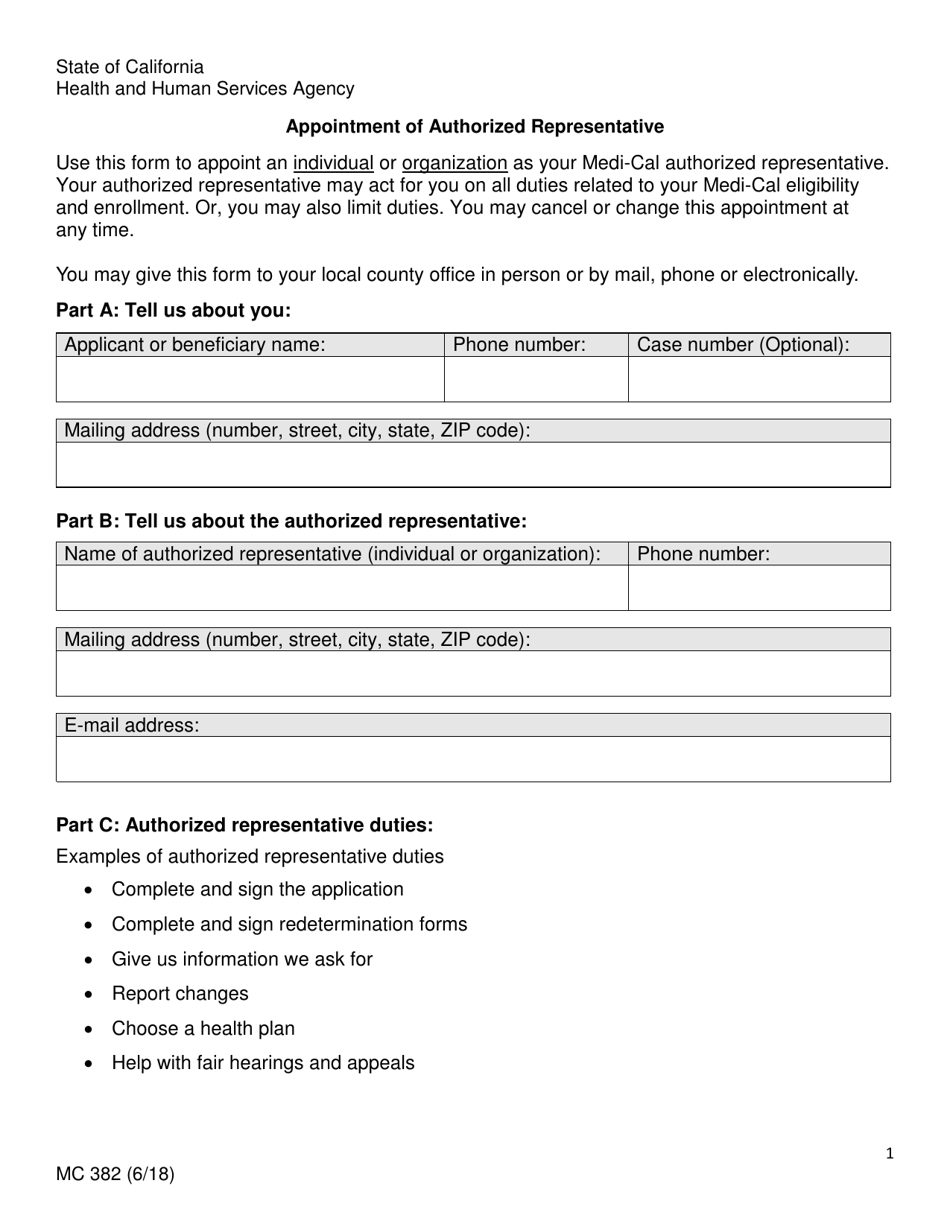
Provide all requested verifications before my Medi-Cal eligibility can be determined. Appointment of Authorized Representative 1. Be sure to select the functions that the representative is being authorized to do.
State of California Department of Social Services. Medi-Cal Access Program MCAP provides pregnant women with co mprehensive coverage for a low cost with no copayments or deductibles for its covered services. Notice of Appointment of Authorized Representative MC 380.
This website provides important information for all Medi. MCAP is for middle-income families who do not have health insurance and whose income is too high for no-cost Medi-Cal. Otherwise referred to as Appointment Form MC 382 or MC 382 in this ACWDL.
In this form the words me or my include my Authorized Representative if I have one. You must complete and mail a signed Authorized Representative. Information SecurityPrivacy Ofce PO.
Complete work registration forms. The policy is based on a review of available clinical information including clinical outcome studies in peer. You may cancel or change the appointment of your Medi-Cal Dental authorized representative at any time.
Or you may also limit duties. Authorization for Release of Information and Appointment of Authorized Representative for Medicaid ApplicationsReviews and Appeals Name of Medicaid applicantmember Social Security Number Appointing an Authorized Representative Mail your signed form to. Sign MC 220 Authorization for Release of Medical Information.
C 382 618 Use this form to appoint an individual or organization as your Medi-Cal authorized representative. Back to Forms By Program. Use this form to appoint an individual or organization as your Medi-Cal Dental authorized representative.
You can fnd the Authorized Representative form on the Medi-Cal Dental website. Welcome to the Medi-Cal Provider Home. Appointment of Authorized Representative form MC 382.
The Counselor will make sure my Personally Identifiable. SCDHHS - Central Mail PO Box 100101 Columbia SC 29202-3101 Fax. This form must be signed by you as the member and submitted to the Medi-Cal.
The Counselor will tell me about all coverage choices I may qualify for including Covered California Health Plans Medi-Cal and the Medi-Cal Access Program. DESIGNATION OF AUTHORIZED REPRESENTATIVE FORM I _____ hereby authorize the following person or company to be Name of applicant my authorized representative in my application for Medicaid filed with the eligibility Determining. Their newborns may be covered by the Medi-Cal Access Infant Program.
Medi-Cal Dental Program Authorized Representative Standard Agreement for Organizations Form. Medi-Cal Dental Program Attn. Where can I fnd the Authorized Representative form.
With the new forms notices and policies for the designation of a Medi-Cal authorized representative AR and to provide instruction regarding these forms. Under the guidance of the California Department of Health Care Services the Medi-Cal fee-for-service program aims to provide health care services to about 13 million Medi-Cal beneficiaries. You may cancel or change this appointment at.
PDF fill and print forms may be completed online and printed to hardcopy to be signed and mailed in or submitted in person to an eligibility. The Counselor cannot choose or recommend a health plan for me. Some links on this page are documents in Adobe Acrobat Portable Document Format PDF.
Unless indicated are smaller than 2 MB. And accept any consequences of the authorized representatives actions as I would my own. Your authorized representative may act for you on all duties related to your Medi-Cal eligibility and enrollment.
AUTHORIZED REPRESENTATIVE FOR HEALTH COVERAGE State Form 55366 R2 12-14 DFR 2123HC Section 1 If you want someone to act on your behalf in applying for benefits andor act for you on an ongoing basis this form must be completed. I UNDERSTAND THAT I HAVE THE RIGHT TO. You can select more than one representative and choose the same or.
 Free 8 Sample Authorized Representative Forms In Ms Word Pdf
Free 8 Sample Authorized Representative Forms In Ms Word Pdf
 Dpss Authorized Representative Form Fill Online Printable Fillable Blank Pdffiller
Dpss Authorized Representative Form Fill Online Printable Fillable Blank Pdffiller
Https Www Dhcs Ca Gov Formsandpubs Forms Forms Mced Mc Forms Mc382 0618 Pdf
 Free 8 Sample Authorized Representative Forms In Ms Word Pdf
Free 8 Sample Authorized Representative Forms In Ms Word Pdf
 Authorized Representative Form For Medical Fill Online Printable Fillable Blank Pdffiller
Authorized Representative Form For Medical Fill Online Printable Fillable Blank Pdffiller
 Free 8 Sample Authorized Representative Forms In Ms Word Pdf
Free 8 Sample Authorized Representative Forms In Ms Word Pdf
Https Www State Nj Us Humanservices Dmahs News Nj Medicaid Designation Of Authorized Representative Pdf
 Medicaid Authorized Representative
Medicaid Authorized Representative
Https Www Dhcs Ca Gov Formsandpubs Forms Forms Mc306 Pdf
Https Forms In Gov Download Aspx Id 5719
 Medicaid Authorized Representative Form Awesome Hipaa Form Consent Top Templates Pliance Patient In Spanish Pdf Models Form Ideas
Medicaid Authorized Representative Form Awesome Hipaa Form Consent Top Templates Pliance Patient In Spanish Pdf Models Form Ideas
 Authorized Representative Form Sample Fill Online Printable Fillable Blank Pdffiller
Authorized Representative Form Sample Fill Online Printable Fillable Blank Pdffiller
 Form Mc306 Download Fillable Pdf Or Fill Online Appointment Of Representative California Templateroller
Form Mc306 Download Fillable Pdf Or Fill Online Appointment Of Representative California Templateroller
 Form Mc382 Download Fillable Pdf Or Fill Online Appointment Of Authorized Representative California Templateroller
Form Mc382 Download Fillable Pdf Or Fill Online Appointment Of Authorized Representative California Templateroller



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.